By Brooke Bachelor, RN, BSN, OMS-II
 My interest in exploring and working within various health care systems has led me around the world. In each country I visit, I strive to understand the intricacies of each unique health care system, and more specifically, the cultural components of reproductive health care. Having worked with many patients from Mexico during my time as a nurse in the US, I knew an MSFC Reproductive Health Externship (RHE) in Mexico City at Clínica Acompañame de Centro de Atención Integral a la Pareja A.C. was a perfect match for me as a future physician exploring a career as a safe abortion provider, primarily for Spanish-speaking patients.
My interest in exploring and working within various health care systems has led me around the world. In each country I visit, I strive to understand the intricacies of each unique health care system, and more specifically, the cultural components of reproductive health care. Having worked with many patients from Mexico during my time as a nurse in the US, I knew an MSFC Reproductive Health Externship (RHE) in Mexico City at Clínica Acompañame de Centro de Atención Integral a la Pareja A.C. was a perfect match for me as a future physician exploring a career as a safe abortion provider, primarily for Spanish-speaking patients.
BACKGROUND:
According to the Grupo de Información en Reproducción Elegida (GIRE), abortion in Mexico is regulated on a local level, with each state establishing its own rules regarding safe abortion access. Elective abortion through the first trimester has only been legal in Mexico since 2007, and even then, only in the Federal District of Mexico City. To put this in perspective, this means that the area where abortion is legal, safe, and elective only covers about 1% of the country, or as little as is depicted by the area shaded in blue on the map below.
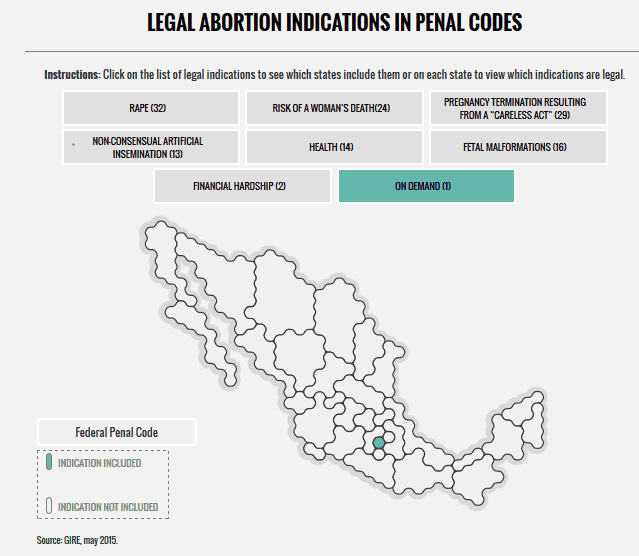
Source: GIRE, May 2015
Unfortunately, this lack of access to safe and legal abortions directly translates to unsafe abortions being the fourth leading cause of maternal mortality. Mexico, like the US, is failing to provide an adequate amount of safe abortion services to meet the needs and demands of the country’s population.
In all Mexican states, an abortion for a pregnancy resulting from rape is technically legal, but in practice, women’s access to services are often limited. In states like Guanajuato, there are no regulated procedures in place to help a woman access a safe abortion. While learning this, I couldn’t help but think of the parallels between this system and the TRAP laws in the US, where abortion may be legal on paper but difficult to access for a variety of reasons.
As we’ve seen repeatedly in countries around the world, restrictions on abortion do not prevent their occurrence. More than one-third of women receiving a clandestine abortion are expected to have complications that require medical treatment. Of those women, an estimated 25% do not receive the hospital care they need.
EXPERIENCE:
Before the RHE, I firmly believed that safe, legal abortion should be available to women everywhere, but I was unsure of how I would react emotionally to seeing an abortion being performed for the first time. I can tell you that the first time I observed an abortion procedure, I said, “That’s it?” This realization of how simple and safe the procedure is, along with seeing the physician’s ability to change lives for the better in a short period of time, strengthened my desire to do this important work.
I was impressed by the clinic’s comprehensive and holistic approach to patient care. Each patient considering abortion had to go through the same screening steps each time to address their specific needs and to be medically and psychologically cleared for an abortion, whether through medication or surgical procedure.
After an initial consultation, women were counseled about how they came to their decision and were able talk openly about any doubts or reservations alone and/or with significant others and family. I quickly learned while hearing the stories of patients that these were not last-minute decisions women made. If a woman chose medication and the option was available to her given her situation, the process was explained to her. After asking any remaining questions, she took a few medications to start the abortion process and was provided an emergency phone number in the rare case that she needed to contact a doctor. If an women opted for the abortion procedure instead of medications, it usually only took about 15-20 minutes from start to finish, and after about 15 minutes in the recovery area, most women walked out of the clinic to continue their lives.
I was so impressed that the clinic not only provided abortions, but also focused much of its effort and energy on preventing these unwanted pregnancies in the first place with subsidized LARCs (long-acting reversible contraception) and other contraceptive methods. The clinic also offered general women’s health consultations and vasectomies.
LESSONS:
Having witnessed this massive gap between need and provision of safe abortion services in Mexico and all over the world, I feel especially motivated to pursue this career path. Here are a few major learning points and important reminders from my experience at Clínica Acompañame:
- From a more practical and professional standpoint, I left my RHE well-equipped linguistically to work in reproductive health as a physician with Spanish-speaking patients. I learned a lot of Spanish vocabulary for specific medical terms that I didn’t even know yet in English.
- Seeing the difference in patients’ outlooks on life before and after an abortion instilled in me the importance of medical schools exposing students to abortion care, even at a basic level. We have the responsibility as health care professionals, regardless of our personal views, to know what resources are available in our communities and, at a minimum, be informed enough to discuss all reproductive health options with women.
- 55% of pregnancies were unintended in Mexico in 2009, so this highlights the need to focus efforts and funding on the prevention of unwanted pregnancy through education and easy access to affordable LARCs.
- It is imperative that BOTH parties each take responsibility for his or her reproductive potential for contraception to be effective. All too often, this responsibility unfairly falls solely upon the woman.
Even with the victories during the last decade for Mexican women that have led to increased safe abortion access, we can and should do more. We must work together as health care professionals and as a society to make sure abortion is accessible, which will undoubtedly save the lives of countless women. I look at the large gap worldwide between need and access to safe abortion services, and as a future physician, I find myself wondering…if not me, then who?


